Annual survey of biopharmaceutical clients honors the organization for excellence in service.
Lincoln, NE (June 1, 2021) – Celerion is pleased to announce that they are the recipient of the 2021 Life Science Leader annual CRO Leadership Awards in all five award categories. This is the sixth consecutive year that Celerion has so been honored.
Well respected within the pharmaceutical industry, the Life Science Leader yearly awards recognize the winning CRO in five categories: overall capabilities, compatibility, expertise, quality and reliability in meeting the needs of big and small pharma clients alike.
“We especially thank our clients for this recognition and for their continued partnership,” says Celerion CEO Susan Thornton, Ph.D. “Throughout the pandemic we’ve taken prudent steps to keep clients’ clinical development programs on track. No matter how challenging the times, our primary mission remains the same, and that is to help get innovative new drugs to market—thus bettering the lives of people in need around the world. We’re proud to once again be recognized for our success in doing so and we owe this recognition to all Celerion employees who have been instrumental in working hard to continuously meet the needs of our clients,” she added.
Ed Miseta, contributing editor of Life Science Leader and chief editor for the website Clinical Leader, says “Our award winners like Celerion have proven themselves to be the top service providers in each category, as reported to us by industry consumers. The superior work ethic exhibited in consistently meeting the needs of their drug development clients is key.”
About Celerion
Celerion, a global leader in early clinical research services, “Translates Science into Medicine”
with its powerful combination of scientific excellence, medical expertise, and clinical operations experience to give clients the confidence to make fast, accurate decisions about their drug development path during the crucial early development period.
For 50 years, Celerion has provided industry leadership and execution of safety/tolerability, pharmacokinetic, and pharmacodynamics studies in highly controlled clinical environments such as first in-human dose escalation, drug-drug interaction, cardiac safety, bioequivalence and bioavailability, metabolism and excretion program, as well as pharmacokinetic evaluations in patients with impaired renal or hepatic function. Celerion completes the offering with data management, biostatistics, clinical monitoring, and bioanalytical services. Our founding mission is to help our clients get their drugs to market quickly so that they touch the lives of our families, friends, and people in need around the world. For more information, please visit www.celerion.com.
Older adults, defined as 65 years of age and up, currently represent ~17% of the general US population and is expected to rise to one-fifth of the population by 2030. Considered a ‘special population’ in the drug development, older adults may hold a greater risk of adverse drug effects due to multiple comorbidities and polypharmacy. A CDC study found that 64% of older adults have two or more chronic conditions, and an estimated 30-35% of older adults take 5 or more prescription medications, which increases the risk of drug-drug interactions. Furthermore, during clinical development safety signals in older adults may differ from younger counterparts. Special attention should be paid to signs of dizziness, delirium, osteoporosis, falls, sedation, bleeding, urinary retention, and loss of appetite.
Ageing and Drug Metabolism
Ageing can significantly affect drug metabolism. A classic example is the reduction in glomerular filtration resulting in lower kidney function typically observed with increasing age, which may require drug dose adjustment for some medications. Other physiological changes include reduced drug absorption; a decrease in muscle mass and increased adiposity can affect drug distribution; as well as lower phase I and phase II enzyme capacity can result in metabolism alterations. Add this to multiple comorbidities and polypharmacy, and there may be a significant shift to the benefit-risk assessment for a new drug in development.
These issues were highlighted in a recent FDA Workshop “Roadmap to 2030 for New Drug Evaluation in Older Adults”. The session stressed the importance of safety and efficacy data of new molecular entities in older adults at the time of NDA or BLA submission as well as major barriers facing current trials, such as stringent I/E criteria that often exclude older adults from trial participation and lack of representation in clinical studies.
Clinical Trial Participation
A 2010-2019 landscape study of drug development applications submitted to the FDA presented during the Workshop found major underrepresentation when comparing disease prevalence to clinical trial demographics. For example, heart failure is prevalent in 25% of adults 80+ years old, however this age group was only represented by 5% of clinical trial participants in heart failure drug studies. Similarly, osteoporosis is estimated in 29% of adults 80+ years old, yet clinical studies only enrolled 12% of octogenarians or older in osteoporosis drug trials. On the other hand, when considering all older adult trial participation, the outcome is not so bleak. According to a recent drug trial snapshot, last year the FDA approved 53 new drug applications (including BLA), in which 30% of trial participants were 65 years of age or older.
Chronological vs. Biological Age
The ICH E7 Q&A and FDA guidance recommend geriatric subpopulation safety and efficacy analysis of three groups; 65-74, 75-84, ≥85 years old. The EMA takes this one-step further in a recent reflection paper,emphasizing biological age and patient frailty over chronological age during drug development with a patient-centric approach. Discussed during the Workshop, the Short Physical Performance Battery is one recommended tool to characterize baseline frailty, testing gait, balance and strength in older adults.
Advantages of Enrolling Older Adults in Early Clinical Development
Increasing representation in Phase III trials, removing unnecessary I/E criteria, and coordinating with nursing homes, long-term care facilities and hospices are just a few approaches to enrich a study with this special population. However, prior to initiating studies in this vulnerable group, early clinical data in healthy older adults can provide valuable insight into PK and PD changes compared to younger adults. Armed with clinical data from older adults during Phase I studies can help de-risk programs when designing Phase II and Phase III I/E criteria.
Over the past 10 years, Celerion has completed 14 Phase I clinical studies in geriatric populations for SAD/MAD, safety & tolerability, food effect, DDI trials, enrolling more than 3000 older adult participants. In our vast database of healthy volunteers, we have a sizeable number of older adults owing to large retirement communities in Phoenix area, enriched by the “snowbird” population.
Conclusion
Traditional barriers to enrolling older adults in late stage clinical trials include safety concerns, trial logistics such as number of visits and intensive assessments, as well as hesitancy of this study population. The latter two can be reconciled through thoughtful study design and community partnership and awareness campaigns. Over coming safety concerns may be attained with early phase clinical studies in a healthy geriatric population to de-risk a drug program.
Celerion continues its Celebration of Translating Science into Medicine for over a decade by highlighting how Celerion ScienceSM has contributed to the development of new therapeutics using our core competencies. While Celerion’s inventive spirit began over 50 years ago, our most important contribution to human health is happening right now, against COVID-19.
2020 has been a breakthrough year working with our biopharma clients to rapidly accelerate both vaccine development and therapeutic treatments against COVID-19. The safety of our patients and employees is an integral aspect of bringing all of us Closer to a Cure and Celerion is proud to have created one of the most comprehensive bioanalytical offerings in the industry for COVID-19 testing, with reliable and rapid results for SARS-CoV-2 PCR testing and antibodies against the virus.
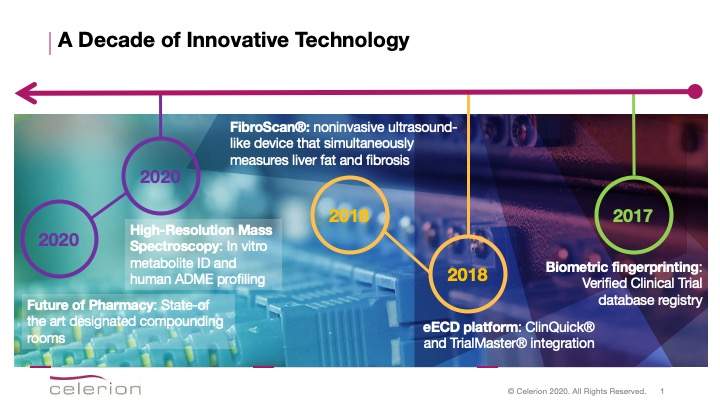
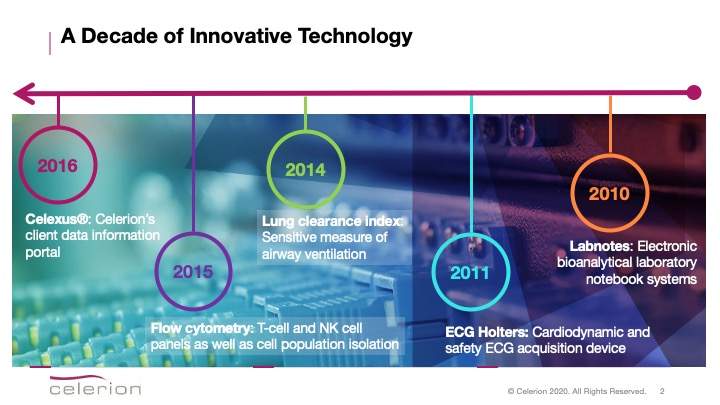
Celerion remains at the forefront of innovative and novel technology to accelerate drug development, deliver high quality data and ensure participant safety. Over the past decade, Celerion has introduced several innovative, High-Tech systems.
Our Top 10 Innovative Technologies Implemented over the Past Decade:
2020 → Celerion delivers the Future of Pharmacy with state-of-the-art pharmacy suites for extemporaneous API compounding. The suites provide dedicated positive and negative pressure rooms for hazardous and non-hazardous material. In addition, the Lincoln pharmacy houses a devoted ADME suite and all Celerion pharmacies are USP <795>, <797>, and <800> compliant.
2020 → The latest enhancement to drug development is high-resolution mass spectrometry (HRMS). HRMS determines the exact mass of molecular ions and is applied in drug development to support in vitro metabolite identification as well as human ADME profiling studies. Our HRMS system is available at our Zurich bioanalytical laboratory.
2018 → FibroScan® is a noninvasive ultrasound-like device that simultaneously measures liver fat and fibrosis. FibroScan® is an integral part of inclusion and exclusion criteria for early phase nonalcoholic steatohepatitis (NASH) studies. Available at our Lincoln, NE and Phoenix, AZ clinics, we have a large database of FibroScan pre-screened participants.
2018 → Celerion provides a fully automated early clinical trial data management platform through the integration of Celerion’s proprietary electronic data acquisition system, ClinQuick®, with OmniComm’s TrialMaster® electronic data capture solution. This integration automates Celerion’s data acquisition system and provides consistent data management and reporting capabilities in one centralized database. It facilitates consistency of data collection across clinical sites, ensuring accurate and high-quality information.
2017 → Celerion uses biometric fingerprint technology to complement Verified Clinical Trials participant database registry. The registry enhances the quality and safety of clinical trials. Biometric fingerprint augments the accuracy and speed of verification as well as adding another layer of protection to ensure dual enrollment in a clinical trial does not occur.
2016 → Celexus® is Celerion’s client data information portal. Clients can access real-time clinical data with operational key performance indicators, a centralized repository for study documentation. The system also features a dynamic interactive experience for analyzing and interpreting clinical data.
2015 → Flow cytometry is a unique bioanalytical service offering. This technique is used to detect and quantify characteristics of a cell population or particles. Flow cytometry can measure T cell and NK cell panels as well as specific cell population isolations (CD cell molecules). Our system even determines simultaneous measurement of multiple cytokine, chemokine, immunoglobulin, or cell signaling targets from a single sample. Immune cell monitoring can be further investigated with ELISpot (enzyme-linked immunosorbent spot). ELISpot is useful to measure B-cell antigen-specific antibodies and T-cell secretion of IFN-γ. This bioanalytical service offering was introduced in 2017.
2014 → Lung clearance index is a sensitive measure of airway ventilation, able to evaluate early signals of efficacy for cystic fibrosis drug development. The system is available at Celerion’s Respiratory Center of Excellence in Belfast, UK, which also houses a dedicated on-site bronchoscopy suite allows bronchoalveolar lavage (BAL), whole-body plethysmography system as well as spirometry apparatuses.
2011 → Celerion’s highly automated ECG core lab uses an ECG acquisition Holter device to collect continuous digital 12-leads ECG recordings for cardiodynamic and safety ECGs. LCD screens optimize data quality by allowing visual inspection of all 12 leads before each collection time point. Digital recordings enable prompt onsite or remote review of safety ECGs to address potential adverse events or subject safety concerns. Using Bluetooth technology, this system was updated in 2015 for direct data capture.
2010 → Workload can be streamlined at the Speed of Science with Labnotes, an electronic bioanalytical laboratory notebook system that comprehensively captures study procedures, observations and results. The system ensures only reagents, solutions, equipment, and prepared standards within quality requirements are used (e.g. expiry, calibration, and preventative maintenance). Data can be reviewed immediately, reducing the chance of errors. Labnotes enables us to meet regulatory requirements for GxP, 21 CFR Part 11, and the FDA’s Electronic Records and Signature Rule.
by Sabina Paglialunga, PhD – Director, Scientific Affairs, Celerion
COVID-19 is a highly infectious respiratory disease caused by the SARS-CoV-2 virus that has affected every corner of the world and nearly all aspects of daily life.In a subset of COVID-19 patients, an exaggerated immune response can lead to acute respiratory distress syndrome (ARDS) requiring mechanical ventilation and leading to death. For society to return to “normal”, it is estimated that ~70% of herd immunity is required [1], which could result in thousands of casualties. Furthermore, this herd immunity target may not be achievable because it is still unknown if those with mild or asymptomatic cases of COVID-19 may not have built up sufficient immunity to prevent reinfection. Therefore, we must consider vaccination as the only viable option to eliminate this virus and thus the race is on to develop an effective vaccine against SARS-CoV-2.
Under the Microscope:
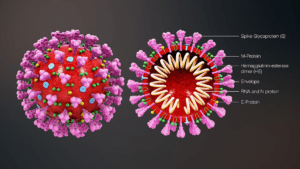
SARS-CoV-2 is a single stranded RNA virus, it is encapsulated by proteins and lipids. The virus has four main structural proteins; a spike glycoprotein (S), a small envelope glycoprotein (E), a membrane glycoprotein (M) and a nucleocapsid protein (N) in addition to other accessory proteins. A homotrimer of S-proteins facilitates binding to angiotensin-converting enzyme 2 (ACE2) receptor on host cells and cell entry [2]. The S-protein is therefore a key site for antibody neutralization, but vaccines developed against other viral protein are also under investigation.
Vaccines 101:
Vaccines boost immunity against infectious diseases through controlled exposure of an antigen, which can be an attenuated virus or fragments of viral proteins.The immune system responds by generating antibodies that protect against future infection. Subsequent exposure to the virus or another infected individual then triggers antibody recognition and the virus is cleared via the immune system activation.Adjuvants are applied to vaccine formulation to upregulate the antigenic response, and depending on the duration of protection, an additional booster shot may be needed.
Vaccine Safety Assessments:
Early clinical phase studies focus on safety, tolerability and immunogenicity, and throughout vaccine development particular attention is paid to hypersensitivity. While vaccines are generally considered safe, serious anaphylactic adverse events associated with immunization can occur, albeit they are extremely rare.Hypersensitivity to the antigen, adjuvants and preservatives have been observed [3] and may require dose adjustment or re-formulation. Another aspect to consider during vaccine development is the potential to induce a Th2 response. Th2 is one of two T-cell responses stimulated when antigens are presented to T cells. The type of T cell response (Th1 vs Th2) results in a particular set of cytokines released. Vaccines depend on a Th1 response to generate immunoglobulins, which elicit immunity against viruses, bacterial and fungal infections. A Th-2 response can counteract Th1 by upregulating interleukin-10 which has anti-inflammatory function [4]. If a Th2-type response is established upon immunization, it can prevent Th1-type response as these are antagonistic processes and a Th2-bias can potentially exacerbate the infection [5].
Bioanalytical Support of Vaccine Trials:
Advanced bioanalytical assays are needed for efficacy and safety measures. It is important that these bioanalytical tests are robust and analytically validated for their context of use in order to support a clinical trial [6].A variety of assays are available for vaccine drug development, which induce antibody titer, qPCR, ELISpot, cell profiling and cytokine biomarkers.
Table 1. Bioanalytical Assays for Vaccine Development
Bioanalytical Assays
Utility
Technology
Antibody titers
Determine the amount of antibodies produced in response to inoculation
Ligand binding methods such as ELISA or MSD
Neutralizing activity of the antibody
Determine the extend in which antibodies can clear the virus
Cell-based assays
Viral load
Determine the presences and amount of virus
qPCR
DNA vaccines
Quantify exogenous viral DNA components
qPCR
mRNA vaccines
Quantify exogenous viral mRNA components
qPCR
T-cell profiling
Examine immune cell populations
Flow cytometry
T-cell response
Examine IFN-γ activation
ELISpot
Antibody producing cells
Evaluate ex-vivo stimulation of PBMC for antibody production
ELISpot
Inflammatory cytokines
Monitor the ‘cytokine storm’ and potential risk stratify for disease severity
Ligand binding methods such as ELISA or MSD
Neutralizing antibodies (NAbs) assay
Antibodies that develop against the biotherapeutic product that can impact it efficacy or safety profile
Cell-based assays
Antibody Dependent Enhancement (ADE)
Characterize the causes of acute lung injury that may occur following coronavirus vaccination
Flow cytometry
Innovative Vaccine Platforms:
There are several platforms for vaccine development.Each technique holds unique advantages and challenges when it comes to safety, manufacturing and scalability [7-9]. The following explores these considerations for the various vaccines under development during the current pandemic.
Whole inactivated and live-attenuated virus vaccines: To create a whole inactivated vaccine, the virus is cultured in a laboratory and then killed (inactivated) or weakened (attenuated) with chemicals, heat, or radiation. This process conserves the virus structure, induces neutralizing antibodies and has been applied for other infectious diseases. There is a risk of hypersensitivity and Th2 bias. In the current crisis, a significant amount of live virus would need to be cultured quickly. Viruses are cultured in cell or egg based media, and these vaccines are contraindicated for individuals with an egg allergy. For recombinant live-attenuated vaccines, parts of the genetic sequence of the virus are manipulated to reduce the virulence. The antigens are produced in the body to facility an immune response. There is potential for the virus to revert to a virulent strain therefore this strategy may not be appropriate to inoculate sensitive populations.
Viral vector vaccines: Weakened adenoviruses or measles viruses are genetically engineered to produce SARS-CoV-2 surface proteins in a patient to elicit an immune response. There is a risk of anti-vector (adenovirus or measles) immunity, lowering the potential immune response against the SARS-CoV-2 target.
Subunit vaccines: Peptide components or fractions of the surface protein antigens are synthesized to create a vaccine.This strategy has a good safety profile however in most cases, subunit vaccines require adjuvants and booster doses.
Virus-like particles: The viral outer shell lacking the genetic material is introduced to patients to trigger a strong immune response. By conserving the virus structure, multiple antigens can be displayed. A caveat of this process is that manufacturing on a large scale may be technically challenging.
Nuclei acid vaccines: DNA or mRNA based vaccines use the patient’s own cell to generate virus peptides and surface proteins that will trigger an immune response (eg. S-protein). The mRNA is encased in a lipid layer that permeates the patients’ cells which act like a bioreactor and transcribe the mRNA into the pathogenic protein that will then stimulate an immune response. DNA vaccines work similarly to mRNA vaccines, with the antigen being coded in a DNA sequence. The DNA is translated to RNA then transcribed to the antigenic peptide. A DNA vaccine does require an extra step to enter into cells, typically with electroporation. One advantage is that more than one viral antigen may be coded. Nucleic acid vaccines are a relatively new technology and have not yet been approved for other infectious diseases.
Table 2. Benefits and Considerations for COVID-19 Vaccine Platforms
Vaccine Type
Benefits
Considerations
Whole inactivated virus
• Conserves viral structure
• Rapid development
• Potential for hyper-sensitivity and Th2-bias
• Culturing live virus
Live-attenuated recombinant virus
• Site-directed attenuation
• Potential to revert to virulent strain
• Not suitable for sensitive populations
• Increase the safety profile; non-integrating
• Egg and cell free
• Rapid, inexpensive and scalable manufacturing
• May suffer from instability
• Low immunogenicity
DNA vaccines
• Non-infectious
• Egg and cell free
• Greater stability
• Potential for multiple antigens
• Rapid production
• Specialized delivery system required
• Potential for integration into human genome
• Low immunogenicity
Adapted from: Zhang et al. 2019 [8] & Prompetchara et al. 2020 [9].
A Coordinated Effort:
The urgency of developing, validating and disseminating a COVID-19 vaccine is palpable. Nearly 100* sponsors have shifted resources and pivoted to the COVID-19 indication. Regulatory agencies are even cutting red-tape to expedite clinical trials. The MHRA approved a COVID-19 vaccine trial in 7 working days. In addition, regulatory authorities have also been swift to implement a series of guidance documents to support sponsors and CROs. Recently, the FDA issued guidance on development and licensure of vaccines to prevent COVID-19. In Europe, similar guidelines have been released by EMA and MHRA. Moreover, countries worldwide are ramping up production of syringes, vials and related paraphernalia needed to inoculate millions once a vaccines is approved. This level of swift global coordination has not been seen before.
Ending the Pandemic:
To end the COVID-19 health crisis quickly, we’ll need more than one solution.Biotech and pharma sectors as well as regulatory agencies and CRO stakeholders are up to the challenge as the race for a vaccine is well underway. Promising early results from vaccine developers such as the University of Oxford with a viral vector vaccine, and Moderna with an mRNA vaccine, are hopeful signs that relief is on its way.With a number of different types of vaccines under investigation, this increases our chances of developing several safe and effective COVID-19 vaccines.
2. Walls AC, Park YJ, Tortorici MA, Wall A, McGuire AT, Veesler D. Structure, Function, and Antigenicity of the SARS-CoV-2 Spike Glycoprotein. Cell. 2020;181(2):281-92 e6.
3. McNeil MM, DeStefano F. Vaccine-associated hypersensitivity. J Allergy Clin Immunol. 2018;141(2):463-72.
4. Berger A. Th1 and Th2 responses: what are they? BMJ. 2000;321(7258):424.
5. Rosenthal KS, Zimmerman DH. Vaccines: all things considered. Clin Vaccine Immunol. 2006;13(8):821-9.
6. Kar S, Islam R. Rapid and robust bioanalytical assays are critical for SARS-CoV-2 therapeutic and vaccine development and beyond. Bioanalysis. 2020.
7. Thanh Le T, Andreadakis Z, Kumar A, Gomez Roman R, Tollefsen S, Saville M et al. The COVID-19 vaccine development landscape. Nat Rev Drug Discov. 2020;19(5):305-6.
8. Zhang C, Maruggi G, Shan H, Li J. Advances in mRNA Vaccines for Infectious Diseases. Front Immunol. 2019;10:594.
9. Prompetchara E, Ketloy C, Palaga T. Immune responses in COVID-19 and potential vaccines: Lessons learned from SARS and MERS epidemic. Asian Pac J Allergy Immunol. 2020;38(1):1-9.
*GlobalData search on 01-June-2020. GlobalData, John Carpenter House, UK.
Acknowledgments: Thank you to Celerion scientists Aernout van Haarst, Sumit Kar, Michelle Combs and Lorraine Rusch for editorial assistance.
Biosimilars are not an exact copy but are similar to the originally approved biological product. Following an abbreviated pathway, they demonstrate equivalent PK, toxicity, similarity, and no clinical change compared to the innovator. The goal of a biosimilar is to introduce lower cost alternatives that can help improve patient access to biological treatments.
Celerion is the premier CRO for PK/PD assessments in healthy subjects and small patient groups. Building upon our bioequivalence and bioavailability expertise, we can design appropriate comparative studies to establish biosimilarity with marketed reference drugs that rely on pharmacodynamic biomarkers and potentially avoid larger patient studies.
With a legacy of over 50 years in clinical research, this year marks a decade of translating science to medicine as Celerion.To commemorate our 10-year anniversary, we are highlighting 10 years of Biosimilars experience.
Our Top 10 lists of Biosimilars Turn-Key Programs and Bioanalytical Assays:
Adalimumab: Monoclonal antibody that targets and inhibits tumor necrosis factor α (TNFα) activity. Adalimumab is indicated for rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis, Crohn’s disease, ulcerative colitis, psoriasis, hidradenitis suppurativa, uveitis, and juvenile idiopathic arthritis. Marketed as Humira, the US patent expired in 2016.
Bevacrizumab: Monoclonal antibody that inhibits vascular endothelial growth factor A (VEGF-A). Bevacrizumab is indicated for colon cancer, lung cancer, glioblastoma, and renal-cell carcinoma and age-related macular degeneration.Marketed as Avastin, the patents expired in the US in 2019 and in Europe in January 2022.
Teriparatide:A recombinant 34 amino acid portion of human parathyroid hormone (PTH), indicated for osteoporosis. Originating product, Forteo/Forsteo patent expired in 2019.
(Peg)Filgrastrim: Neupogen is the originator filgrastrim product recombinant granulocyte colony-stimulating factor (G-CSF) indicated for conditions of neutropenia. Neulasta is a pegylated form of filgrastrim. Pegylation increases the half-life and stability. Neupogen patent expired in 2006 in Europe and 2013 is the US. Neulasta patent expired in 2015 and 2017 in the US and EU respectively.
Ustekinumab: Marketed as Stelara, it targets IL-12 and IL-23 and is indicated for plaque psoriasis, Chron’s disease and ulcerative colitis. Patents expires in 2023 in the US and in 2024 in Europe.
Omalizumab: Sold under the brand name Xolair, omalizumab is indicated for asthma and chronic idopathic utricaria. By inhibiting immunoglobulin E from binding to high affinity receptors on mast cells and basophils, omalizumab reduces sensitivity to allergens.Patent expired in 2017 in the US and Europe.
Ranibizumab: Ranibizumab is a monoclonal antibody fragment that inhibits angiogenesis by inhibiting VEGF-A. It treats age-related macular degeneration, a common source of vision loss with aging. It is also effective in diabetic macular edema. The brand name is known as Lucentis and its patent expires in June 2020 in the US and 2022 in Europe.
Cetuximab: A monoclonal antibody that inhibits epidermal growth factor receptor (EGFR) used for the treatment of metastatic colorectal cancer, metastatic non-small cell lung cancer and head and neck cancer. The patent for the brand name product, Erbitux, expired in 2014 in Europe and in 2016 in the US.
Trastuzumab: Monoclonal antibody, sold under the brand name Herceptin. Trastuzumab is a HER2 receptor antagonist, indicated for breast and stomach cancers that are HER2 receptor positive. Patents expired in 2014 in the EU and 2019 in the US.
Etanercept: Commonly known as Enbrel, it is a TNFα inhibitor that functions as decoy receptor for the cytokine. Etanercept is indicated for various rheumatic and psoriatic disorders. US patent is extended to 2028, however the patent is expired in EU and biosimilars are available in this region.
Lincoln, Neb.; June 16, 2020 (Business Wire) – Celerion is proud to announce, for the fifth consecutive year, recognition of its early stage research development services across five categories in the 2020 CRO Leadership Awards sponsored by Life Science Leader and Industry Standard Research.
Both small and large pharma respondents highlighted Celerion as a top performer in categories including Capabilities, Compatibility, Expertise, and Quality. Importantly, small pharma respondents overwhelmingly recognized Celerion as a Leadership Champion for Reliability.
“It is very meaningful to receive the recognition across multiple categories, but to stand out as a reliable partner is most important. These awards coincide with our 10-year anniversary of Celerion’s formation — what we refer to as “A Decade of Translating Science into Medicine,” said Susan Thornton, Ph.D., Celerion CEO. ” Celerion has achieved global recognition as the premier provider of early stage clinical research, building upon the legacy of our predecessor, Harris Laboratories, where clinical pharmacology research services were initiated over 50 years ago. Now more than ever, Celerion’s employees are motivated every day by knowing that their work impacts the delivery of new medicines that touch the lives of our friends, families, and people in need around the world affected by the current Covid-19 pandemic.”
Ed Miseta, executive editor, Life Science Leader, added, “We believe the CROs receiving an award this year are truly at the top of their class and are deserving of this recognition. Being a top performer in any of these categories shows a level of expertise and commitment to clinical trials and serving the needs of biopharmaceutical companies and their patients.”
About Celerion Inc.
Celerion, a global leader in early clinical research services, “Translates Science into Medicine” with its powerful combination of scientific excellence, medical expertise, and clinical operations experience to give clients the confidence to make fast, accurate decisions about their drug development path during the crucial early development period.
For 50 years, Celerion has provided industry leadership and execution of safety/tolerability, pharmacokinetic, and pharmacodynamics studies in highly controlled clinical environments such as firstin-human dose escalation, drug-drug interaction, cardiac safety, bioequivalence and bioavailability, metabolism and excretion program, as well as pharmacokinetic evaluations in patients with impaired renal or hepatic function.
Celerion completes the offering with data management, biostatistics, clinical monitoring, and bioanalytical services. Our founding mission is to help our clients get their drugs to market quickly so that they touch the lives of our families, friends, and people in need around the world. For more information, please visit www.celerion.com.
The global COVID-19 pandemic has altered the mechanics of nearly every industry. For early phase clinical trials, adapting to this crisis has led to augmented risk mitigation procedures and greater use of innovative technology. Since continuity of your drug program is important to you, the patients in need of these therapies, it is important to us.
We have taken a proactive approach to conducting business, now when research is needed more than ever. Our strengths lie in being flexible and nimble, which is a benefit during times of uncertainty.
Our ‘New Normal’ is built on three key pillars; Safety, Resources and Communication.
Safety First
The health and safety of our participant and staff is of the utmost importance. We have incorporated several measures to screen, clean and isolate for COVID-19 virus during trial operations. We are following all CDC, FDA and MHRA guidelines as well as local regulations for clinical operations during the COVID-19 pandemic.
Health Checks: All participants, staff and visitors will have their temperature checked and queried about COVID-19 symptoms or contact with positive patients upon entering Celerion facilities. Access will be denied to anyone showing symptoms of the disease.
PPE: All participants, visitors and staff will wear appropriate PPE while at the Clinic.
COVID-19 Testing: Regular PCR screening for virus detection and antibody testing for potential immunity will be performed.
Cleaning: Amplified cleaning measures have been put in place with special attention being paid to high-touch areas. Regular hand washing is encouraged for all participants and staff, and hand sanitizer is available at facility entry points and throughout the building.
Social Distancing: Isolation and distancing procedures are now in place. Participants will E-consent prior to screening and experience staggered screening as well as segregation in the clinic. Staff are instructed to work within their zoned areas, maintain 6 ft. social distance as much as possible, limit face-to-face interactions and time spent in common areas.
Testing, Testing, Testing! Celerion Bioanalytical Services has focused capabilities on COVID-19 screening by PCR, viral load quantification, antigen detection, antibody titer measurement, cell-mediated immunity assessments as well as cytokine and chemokine inflammation biomarker assays.
We Lead Quality
We have the essential resources in place to safely and effectively execute your clinical trial.
Supply Chain: We have secured the necessary PPE for our staff and participants.
Celerion Express:New screening facility located at the Nebraska Innovation Campus.
Bed Capacity and Space: 3 Clinical Pharmacology Units – 600 bed capacity
Enough beds to accommodate social distancing during participant confinement
Recruitment: Robust database of +130 000 participants
Experienced Workforce: +1000 Employees
Thoroughly trained Clinical Associates
Medical and Subject Matter Experts
Clinical Pharmacology team with expertise in study design, data analysis, interpretation and medical writing
Knowledgeable Bioanalytical Scientists
Communication is Key
With conditions rapidly changing, effective communication among all stakeholders is critical.
Response Plan: A Celerion Pandemic Management Plan is distributed to our clients prior to study start. This report outlines risk mitigation steps, training procedures and screening activities.
Adapting to Regulatory Guidance: We are in regular communication with IRB and IEC, and we are quickly disseminating and incorporating FDA, EMA, MHRA guidance regarding the COVID-19 pandemic.
Leveraging technology: We engage innovative tools to support virtual meetings and remote data review. Our clients are provided with real time data accesses through our Celexus® system.
Celexus® is Celerion’s client data portal. It is an information hub with real-time access to safety data and trial progress dashboard.
During this dynamic situation, the steps we have put in place for the safety of participants and staff, securing supply chain and innovative technology are designed with one objective in mind, to help our biotech and pharma partners get their products to market faster.
 by Sabina Paglialunga, PhD – Director, Scientific Affairs, Celerion
by Sabina Paglialunga, PhD – Director, Scientific Affairs, Celerion